Healthcare · Customer Experience
Customer Service Automation for Healthcare Providers: AI-Native, Trust-First
We design, build, and run AI-native customer service automation for hospital systems, clinics, care operations leaders, and patient access teams. This page describes the engagement: scope, pricing, timeline, controls, and the KPIs we commit to.
Projects from $15k · Refundable 7 days · Kickoff within 5 days
Early access: we work with a small first cohort. Engagements are scoped, priced, and shipped end-to-end by our team — not referred to third parties.
In one sentence
AI-native customer service automation for healthcare providers — From Discovery baseline to production traffic in 8-12 weeks, with the operating model — eval harness, reviewer UI, audit log, calibration cadence — handed over as part of Build, not deferred to Run. Expected delta on first contact resolution: −99.7%.
Key facts
- Industry
- Healthcare Providers
- Use case
- Customer Service Automation
- Intent cluster
- Customer Experience
- Primary KPI
- first contact resolution, support cost per case, CSAT, and backlog age
- Top benchmark
- Median response time: 4h 22min → 47s (−99.7%)
- Systems integrated
- EHR, RCM, patient portals
- Buyer
- hospital systems, clinics, care operations leaders, and patient access teams
- Risk lens
- patient safety, clinical validation, privacy, consent, and equity
- Engagement timeline
- Discovery 2 weeks → Build 9 weeks → Run continuous (integration-heavy)
- Team size
- 1 senior delivery + 1 part-time domain SME
- Discovery price
- $5k · 2-week sprint
- Build price
- $18k–$25k · 6-9 weeks
Primary outcome
reduce support volume while improving response quality
What we ship
AI service desk, escalation paths, knowledge workflows, and quality dashboards
KPIs we report on
first contact resolution, support cost per case, CSAT, and backlog age
Why Healthcare Providers teams hire us for this
Healthcare Providers runs on EHR, RCM, patient portals and adjacent systems. Most automation projects in this space stop at integration — they move data, but they do not change how decisions are made. AI-native customer service automation starts from the decision itself: which step needs evidence, which step needs judgment, which step can run unattended once governance is in place.
Zendesk and Salesforce CX research show that healthcare providers customers tolerate AI-assisted service when the escalation path to a human is fast and obvious. We design the escalation surface before we design the automation.
Industry context: Mid-market and enterprise operators face the same fundamental tradeoff: AI must compress operational cycle time while remaining auditable and integrable with existing systems of record.
Benchmarks we hit
Reference benchmarks from production deployments of customer service automation in healthcare providers-comparable contexts. Sources noted per row. Your actuals are measured against the baseline captured in Discovery.
| Metric | Industry baseline | AI-native typical | Delta |
|---|---|---|---|
Median response time AI handles 80% of intents; humans handle the 20% that need judgment | 4h 22min | 47s | −99.7% |
Support cost per case (fully loaded) Includes AI tokens, agent time, QA review, infra overhead | $8.40 | $2.10 | −75% |
CSAT (post-interaction) Lift requires escalation paths kept obvious and fast | 4.1 / 5 | 4.4 / 5 | +0.3 |
Benchmarks are reference values from comparable engagements and authoritative sector benchmarks. Your engagement's baseline is captured during Discovery and actuals are reported weekly during Run against that baseline.
How we operate the workflow
A traditional agency sells people, hours, and deliverables. We sell a designed outcome. For customer service automation, the operating model includes intake, data access, prompt and retrieval architecture, workflow orchestration, evaluation, human review, reporting, and continuous improvement. The human role stays central: review edge cases, own sensitive escalations, coach the knowledge base, and approve policy changes. In healthcare providers, where the risk lens covers patient safety, clinical validation, privacy, consent, and equity, that separation matters.
What we build inside the workflow
For healthcare providers workflows, the design choice that matters most is where to draw the boundary between automation and human judgment. On customer service automation, we draw three lines: full automation (high-confidence, low-stakes, reversible actions), assisted review (drafts with reviewer one-click approval), full human ownership (policy edits, escalations, exceptions). The lines are documented, instrumented, and revisited quarterly as confidence calibration improves.
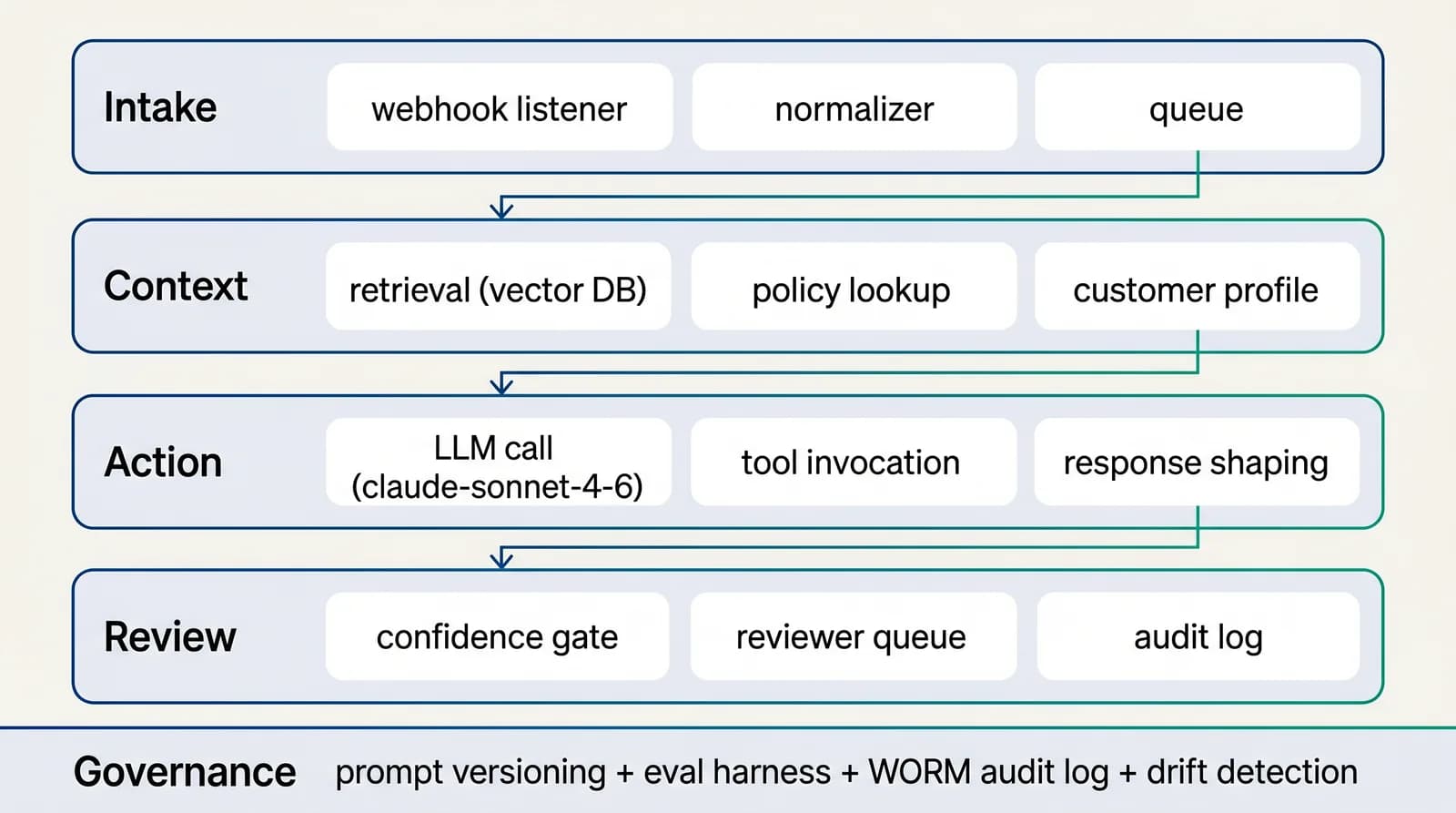
Reference architecture
4-layer AI-native workflow for customer experience
The architecture is designed for substitution: any single layer (model, retrieval store, reviewer UI, action client) can be swapped without rewriting the others. That is the property that lets customer service automation survive 12+ months of provider and pricing change.See the full architecture diagram for Customer Experience →
AI-native vs traditional approach
What changes between a traditional customer service automation program in healthcare providers and an AI-native engagement is not the goal — it is the architecture, the operating cadence, and the exit posture. The table below makes the differences explicit.
| Dimension | Traditional (in-house build or BPO) | AI-native engagement (us) |
|---|---|---|
| Lead time to live deployment | 6-12 months | 6-10 weeks (thin slice) |
| Engagement billing | Time-and-materials or annual contract | Phased fixed-price (Discovery → Build → opt Run) |
| Audit posture | Manual logs, periodic review | Versioned prompts, audit logs, reviewer queues, attestations |
| Per-operator capacity | 1.0× (baseline) | −75% |
| Per-case cost | Industry baseline | Sub-dollar marginal cost on routine envelope |
| Exit path | Knowledge transfer takes 6+ months | Documented exit at every phase; artefacts in your repo |
Traditional process automation projects cost $80-200k+ with 6-12 month payback; AI-native engagements deliver thin-slice production in 6-8 weeks with measurable baseline-vs-actuals reporting.
Engagement scope & pricing
Three phases, three commercial envelopes. Discovery is the only commitment to start; Build and Run are scoped against the Discovery output.
CX engagement
Each phase is independently committable. Discovery is the only one you have to start with.
Phase 1 · Discovery
$5k
2-week sprint
Phase 2 · Build
$18k–$25k
6-9 weeks
Phase 3 · Run
$2k–$3k / mo
optional, hourly bank also available
~$28k–$48k typical year 1 (60% take the run option for ~6 months)
Customer journey design, escalation handling, tone calibration, and CX KPI reporting.
The only thing you commit to today is the Discovery sprint. The Build SoW is produced inside Discovery and you decide whether to proceed. Run is optional.
The 4-phase delivery model
Phase 1 · Weeks 1–2
Discovery
We sit with the operator team running the workflow today, watch a working day end-to-end, and produce the baseline that Build will be measured against. Two-week sprint, fixed price.
Phase 2 · Weeks 2–4
Design
We design the operating model: data access, retrieval, prompts, review queues, controls, and the KPI dashboard.
Phase 3 · Weeks 4–8
Build
6-10 week sprint that ships the thin-slice production workflow on top of your existing systems. Eval harness gating every prompt change. Reviewer queue staffed. Audit log queryable. Dashboard live.
Phase 4 · Weeks 8+
Run
Run cadence is calibrated to your operational reality: weekly metric review, bi-weekly prompt refresh, monthly calibration audit, quarterly architecture review. The Run phase compounds value as the labelled test set grows.
Interactive ROI calculator
Estimate your AI-native ROI for customer service automation
Reference inputs below are typical for healthcare providers teams in the customer experience cluster. Adjust them to match your situation.
Projected
Current monthly cost
$42,000
AI-native monthly cost
$13,000
Annual savings
$348,000
69% cost reduction · ~920 operator-hours freed / month
Governance and risk controls
Internal auditors and external regulators in healthcare providers converge on the same three questions: data provenance, decision traceability, replayability. Our control stack answers all three from the same audit log — one source of truth, queryable, exportable, signed. No spreadsheet reconciliation, no after-the-fact narrative.
How we report ROI
The business case lives in operating metrics, not model benchmarks. For customer service automation, the metrics that matter are first contact resolution, support cost per case, CSAT, and backlog age. For Healthcare Providers, leadership will also care about patient access time, denial rate, clinician documentation burden, and care gap closure. Every build decision we make connects to one of those metrics, and we publish a weekly performance review during the Run phase.
Selected portfolio
Real builds — customer service automation in healthcare providers and adjacent sectors
Below are engagements drawn from our active portfolio where the workflow rhymed with customer service automation in healthcare providers or in adjacent contexts. Scope and stack are accurate; client identities are withheld under engagement NDAs.
Q1 2026
AI-powered interior design platform — generative room concepts for the MEA market
AI interior design SaaS · MEA region
Vertical AI SaaS for interior design in the Middle East: image-conditioned generation tuned for local taste profiles, room-by-room concept workflow, project export for designers and clients. Built with a market-specific dataset and an evaluation loop on regional aesthetic baselines.
- Next.js + image generation pipeline
- Regional taste-profile tuning
- Designer + client export flows
Q3 2025
Property marketplace — buy, rent, list across apartments, villas, commercial
Regional real-estate marketplace · GCC region
National real-estate marketplace covering apartments, villas, and commercial property: listing management for agencies and owners, search and filter optimised for local buyer intent, SEO foundation built for long-tail property queries, lead capture per listing with routing to the listing agent.
- Next.js + dynamic SEO routes
- Listing CMS
- Lead routing engine
Q1 → Q2 2026
National legal marketplace — directory, bookings, legal tools, emergency contacts
Government-licensed legal services platform · GCC region
Ministry-licensed bilingual EN/AR platform: directory of certified lawyers, firms, mediators and arbitrators; multi-channel appointment booking (video, phone, in-office); free legal tools (court fees, deadlines, legal interest); police directory with map + hotlines; provider verification workspace; PDF document generation with QR-coded provenance.
- Next.js 16 monorepo (Turborepo)
- Bilingual EN/AR (next-intl)
- Postmark + Web Push
Client identities withheld under engagement NDAs. Sector, geography, and scope are accurate. Full case studies on request.
Common pitfall & mitigation
The failure mode we see most often on AI-native customer service automation engagements in healthcare providers contexts.
Tone mismatch with brand
AI drafts feel generic, brand managers refuse to enable autonomous send
Brand-corpus grounding + tone evals on labelled samples before any autonomous send
Regulatory landscape and how we ship inside it
The single regulatory question that makes or breaks healthcare providers customer service automation engagements is "who is accountable for an automated decision". Our answer, baked into the architecture: there is always a named human owner per decision class, with the role visible in the reviewer interface, the audit log, and the governance map. Full automation does not mean no accountability — it means the named accountable human approved the policy that authorized the automation, and can revoke that authorization at any time without re-architecting the system.
Compliance officers in healthcare providers have seen enough "AI governance frameworks" to recognize when one is theatre. The questions they actually ask are concrete: where does the training or retrieval data come from, who curates it, how do model updates get validated, what happens when the model disagrees with the policy, and how is the operator team trained to override.
We answer each of those concretely in the Build phase. Retrieval data is curated by a named subject-matter expert from your team during Discovery, with a documented refresh cadence and an approval workflow for new sources. Model updates are gated by the evaluation harness: a new candidate model has to beat the incumbent on the labelled test set across multiple metric slices before it is promoted, and the comparison is logged. Policy disagreements surface as escalations, not silent overrides — when the model recommends an action that conflicts with a policy clause, the reviewer queue captures both, the operator decides, and the decision feeds the next iteration of the prompt. Operator training is a deliverable, not an afterthought: we ship the reviewer playbook, the calibration sessions, and the first month of paired-review with your team during the transition out of Build.
The net effect for healthcare providers leadership on customer service automation is a workflow that holds together under the three audiences that matter — internal audit, compliance, supervisor — without requiring three different versions of the story. The dashboard is the story. The audit log is the evidence. The control map is the framework. All three are live, all three are queryable, and all three are designed for the regulated reality your team operates in.
The tactical playbook for the first 30 days
Week 1 — Discovery handover and labelled test set capture. We sit with the operator team running customer service automation today, watch a working day end to end, and capture 200+ real cases as the labelled test set. By Friday we have the workflow map, the system inventory (EHR, RCM, and adjacent), the risk register, and the success metrics aligned with your KPI of first contact resolution.
Week 2 — Architecture and integration scoping. We design the four-layer workflow (intake, context, action, review), confirm the retrieval shape, lock the prompt strategy direction, and produce the integration plan against EHR. The output is the Build statement of work with a fixed price and a named deliverable per phase.
Week 3-4 — Build sprint 1: retrieval and intake. We stand up the retrieval index against your approved sources, build the intake classifier, instrument the audit log, and run the first eval cycle against the labelled test set. The thin slice is functional but not production-deployed.
Week 5-6 — Build sprint 2: action and review. We ship the action layer, build the reviewer queue UI, calibrate the confidence thresholds against the labelled test set, and onboard the first reviewer cohort. By end of week 6 the workflow is processing low-stakes production traffic with full audit logging.
The rest of the Build phase widens the production envelope case-by-case based on the reviewer feedback loop. By the end of Build, customer service automation for healthcare providers is running on real traffic with the operating cadence already established.
The Build phase rhythm for customer service automation in healthcare providers is engineered for the bottleneck most teams hit at the end of week 2: ambition outrunning evidence. We engineer for the opposite — evidence first, ambition calibrated to it.
Week 1 produces the discovery report, the labelled test set, the integration plan, the risk register, the success metrics. Week 2 stands up the retrieval index, the intake classifier, the eval harness, the audit log. Week 3 wires the action layer with reviewer approval, runs the first three eval cycles, produces the first calibration report. Week 4 ships the thin slice to a narrow production audience (5-10% of routine cases), instruments the operator feedback loop, and runs the first weekly review.
By day 30, the dashboard is live, the system is processing real healthcare providers cases, the operator team is engaging with the reviewer queue, the eval harness is gated on every change, and the next two weeks of Build are scoped from concrete evidence rather than initial assumptions. Days 31-45 widen the production envelope to 40-60% of routine cases. Days 46-60 absorb the remaining routine envelope and start handling the first tranche of exceptional cases. By the close of Build (day 60-70), the workflow is operating at its target envelope with the calibration discipline in place to handle drift, edge cases, and future model changes.
How this rhymes with a recent build
A comparable engagement worth knowing about for customer service automation in healthcare providers is summarised below. Identity withheld under engagement NDA; sector and stack are accurate.
Property marketplace — buy, rent, list across apartments, villas, commercial. National real-estate marketplace covering apartments, villas, and commercial property: listing management for agencies and owners, search and filter optimised for local buyer intent, SEO foundation built for long-tail property queries, lead capture per listing with routing to the listing agent. (Regional real-estate marketplace · GCC region, Q3 2025.)
The reason that engagement is a useful reference is not the surface match — it is the underlying decision structure. The same questions show up on customer service automation for healthcare providers: where to draw the automation boundary, how to calibrate confidence thresholds against the labelled test set, what to put in the reviewer UI, how to instrument drift. The answers transfer; the implementation specifics adapt to your stack.
For US buyers
US compliance scaffolding for customer service automation in healthcare providers (HIPAA, PHI, NIST AI RMF)
Healthcare Providers engagements touching US clients on customer service automation ship with the regulatory scaffolding your procurement, compliance, and legal teams expect. The framework that matters most for healthcare providers is Health Insurance Portability and Accountability Act (HIPAA) — addressed below alongside the adjacent frames we encounter.
HIPAA
Health Insurance Portability and Accountability Act
Authority: U.S. Department of Health and Human Services / OCR
- Scope
- Protected Health Information (PHI) handling, security safeguards, breach notification, business associate accountability.
- How we ship inside it
- We sign a Business Associate Agreement (BAA) on healthcare engagements that touch PHI. The architecture supports BAA-covered model providers (Anthropic BAA, Azure OpenAI BAA, AWS Bedrock BAA). Audit log retention defaults to 6 years (HIPAA minimum). PHI handling follows minimum-necessary principle at the prompt and retrieval layers.
PHI
Protected Health Information
Authority: HIPAA Privacy Rule
- Scope
- Any health information that can identify an individual.
- How we ship inside it
- PHI is redacted before transmission to non-BAA model providers; retention follows BAA terms; access is logged at the user level. Workflows touching PHI are deployed to BAA-covered infrastructure only.
NIST AI RMF
NIST AI Risk Management Framework (AI 100-1)
Authority: U.S. National Institute of Standards and Technology
- Scope
- Voluntary framework: Govern, Map, Measure, Manage functions for AI system risk.
- How we ship inside it
- Every engagement maps to NIST AI RMF during Discovery. The control map produced becomes the artefact your internal audit and security teams use to defend the workflow.
For US companies
Start a US-friendly engagement
Discovery from $8,500–$12,000, Build from $35,000–$75,000, optional Run from $5k/mo. Fixed-price, milestone-billed, you own every artefact. Send a short brief and we reply within 5 business days. 11am–4pm ET overlap for live syncs.
USD pricing
Discovery $8,500–$12,000 · Build $35,000–$75,000
US-style commercial
MSA / SOW / mutual NDA standard. DPA with SCCs included.
Limited capacity
We onboard 3–5 new clients per quarter to protect delivery quality.
Build internally or work with us
Some healthcare providers teams should build internally, especially when they already have strong product, data, security, and operations capacity. Most teams move faster with us because the bottleneck is not only engineering — it is translating messy operational work into a reliable AI-assisted workflow that people will actually use. After 6 to 12 months you can absorb the operating model internally or keep us as a managed execution partner.
What to ask us before signing
- Ask for a 30/60/90-day plan with named deliverables, not a vague phase description.
- Ask how we handle the long tail of edge cases the operator team has never encoded — escalation, calibration, capture.
- Ask for the model and provider strategy — single-model, multi-model, fallback paths, cost forecasting.
- Ask how the reviewer queue UX is designed and whether your operator team can shape it during Build.
- Ask for references from healthcare providers-adjacent engagements — sector, scope, and outcome dimensions.
Recommended first project
Our recommendation for a first customer service automation engagement in healthcare providers is to pick the slice of the workflow that satisfies four criteria: there is a measurable baseline, the work is genuinely repetitive, the failure mode is reversible within a reasonable window, and a senior operator on your team can be the first reviewer. Those four criteria filter out the engagements that look impressive in a slide and fail in week three. The 90-day target is "thin slice in production with a defended baseline". By day 30, the system processes a small share of real traffic with full reviewer oversight. By day 60, the share has widened and the calibration is data-driven. By day 90, the operating cadence is your team's, the dashboard reflects empirical performance, and the case for the next workflow writes itself.
Frequently asked questions
How do you automate customer service automation in healthcare providers with AI?+
We map the existing customer service automation workflow inside healthcare providers, identify the high-volume, high-structure tasks, and build an AI agent that handles those tasks while routing low-confidence cases to a human reviewer. The build connects to your EHR, RCM, patient portals, runs against a labelled test set, and ships behind a reviewer queue before it sees production traffic. We then operate it, measure first contact resolution, support cost per case, CSAT, and backlog age, and improve it weekly.
What does it cost to automate customer service automation for healthcare providers teams?+
~$28k–$48k typical year 1 (60% take the run option for ~6 months). The structure: $5k Discovery (2-week sprint) → $18k–$25k Build (6-9 weeks) → optional $2k–$3k / mo Run. Customer journey design, escalation handling, tone calibration, and CX KPI reporting.
What is the best AI agent for customer service automation in healthcare providers?+
Model selection on customer service automation for healthcare providers happens against five criteria: quality on your labelled test set, cost per inference at your projected volume, latency budget for the user-facing path, provider reliability over 12-18 months, contractual data-handling posture. We bring the comparative methodology from prior engagements and run it during Build; the winning model is the one that survives all five, not the one that wins the demo.
How long does it take to deploy AI customer service automation for healthcare providers?+
A thin-slice deployment in 2-week sprint after Discovery, with real healthcare providers data and real reviewers. The full Build phase runs 6-9 weeks. By day 90, first contact resolution, support cost per case, CSAT, and backlog age is instrumented, the team has a baseline, and leadership has the data needed to decide on expansion into adjacent healthcare providers workflows.
What do we own, and what do you own?+
What we ship as code lives in your repository under your IAM. The prompts, the evaluation harness, the integration code, the reviewer UI, the infrastructure-as-code — all in your Git, not in our SaaS. We bring the engineering, the operating discipline, and the cadence; you bring the data, the policy, and the operator team. The handover is documented from day one of Build, not deferred to the end.
How do you protect customer trust when AI handles customer service automation?+
We design tone, escalation, and confidence thresholds with your CX leaders. Low-confidence interactions route to humans, and we track first contact resolution, support cost per case, CSAT, and backlog age alongside qualitative review.
Do you train models on our data?+
No. We do not train any model on client data. Anthropic Zero-Data-Retention is enabled by default; OpenAI default-no-training is honoured. Prompts, retrieval indexes, audit logs, and integration data live in your cloud account under your IAM. At engagement end, every artefact transfers to your repository.
What if we want to exit the engagement?+
Discovery and Build are fixed-scope, so there is no mid-engagement exit cost. Run is month-to-month with 30-day notice. Every artefact (prompts, eval harness, integration code, dashboards, runbooks) is in your repository throughout the engagement, not behind our SaaS. There is no lock-in.
What does success look like 90 days after Build closes?+
first contact resolution, support cost per case, CSAT, and backlog age measurably improved against the Discovery baseline. Your team is operating the workflow with the cadence we shipped during Build. The audit log is queryable. The reviewer queue is calibrated. The next workflow scope is informed by real production evidence rather than initial assumptions.
What support is included after the engagement ends?+
Optional Run retainer covers weekly cadence, prompt refresh, retrieval index updates, and reviewer-queue calibration. Architecture-level questions and breaking-change support are billed hourly outside of Run. Most engagements transition Run in-house at month 6-12; we stay available for architecture decisions for 12 months at no extra charge.
How does this integrate with EHR and our existing stack?+
Discovery scopes the integration footprint explicitly. We integrate at the API layer; no replatforming required. The Build statement of work names exactly which systems are connected, which data flows are bidirectional, and what authentication patterns we use (SSO, service accounts, OAuth scopes). The integration code lives in your repository.
What does your team look like during an engagement?+
Discovery: 1 senior delivery lead + 1 PM, ~30 hours/week. Build: 1 senior delivery lead + 2-3 senior AI engineers, ~50-80 hours/week across the team. Run: 1 delivery owner + 1 engineer on weekly cadence. We do not use offshore staff augmentation. Every engineer touching your engagement is senior-level.
Sources we reference
The following sources inform the architecture, governance, and benchmarks we apply on healthcare providers engagements. Cited here so you can verify and dig deeper.
- WHO Artificial Intelligence for Health
- Hype Cycle for Artificial Intelligence — Gartner
- MIT Sloan Management Review — AI & Business Strategy — MIT Sloan
- State of the Connected Customer — Salesforce Research
- Customer Service & AI — Zendesk CX Trends
- Google Search Central: helpful, reliable, people-first content
- Google Search Central: URL structure best practices
High-intent reads
Start the engagement
Start a Healthcare Providers engagement
Tell us about your workflow, the systems involved, and the KPI you want to move. We'll send a scoped statement of work within 5 business days.