Healthcare · Knowledge & Insight
How to Automate Knowledge Management in Healthcare Providers (Step-by-Step)
hospital systems, clinics, care operations leaders, and patient access teams usually arrive here with two questions: what does AI-native knowledge management actually ship, and what does it cost. Both are answered below, alongside the operating posture and the governance frame.
Projects from $15k · Refundable 7 days · Kickoff within 5 days
Early access: we work with a small first cohort. Engagements are scoped, priced, and shipped end-to-end by our team — not referred to third parties.
In one sentence
AI-native knowledge management for healthcare providers — A phased engagement that ships a production knowledge management workflow on top of EHR and RCM, moves the operating metric against a Discovery-captured baseline, and is operated under explicit governance from day one. Expected delta on search success: +62 pts.
Key facts
- Industry
- Healthcare Providers
- Use case
- Knowledge Management
- Intent cluster
- Knowledge & Insight
- Primary KPI
- search success, time saved, knowledge freshness, and repeated question reduction
- Top benchmark
- Source citation completeness: 38% → 100% (+62 pts)
- Systems integrated
- EHR, RCM, patient portals
- Buyer
- hospital systems, clinics, care operations leaders, and patient access teams
- Risk lens
- patient safety, clinical validation, privacy, consent, and equity
- Engagement timeline
- Discovery 3 weeks → Build 8 weeks → Run continuous (regulated industry)
- Team size
- 2 senior delivery + 1 part-time reviewer trainer
- Discovery price
- $6k · 2-week sprint
- Build price
- $22k–$30k · 7-10 weeks
Primary outcome
make institutional knowledge searchable and actionable
What we ship
knowledge graph, retrieval assistant, content governance, and freshness workflow
KPIs we report on
search success, time saved, knowledge freshness, and repeated question reduction
Why Healthcare Providers teams hire us for this
Healthcare Providers runs on EHR, RCM, patient portals and adjacent systems. Most automation projects in this space stop at integration — they move data, but they do not change how decisions are made. AI-native knowledge management starts from the decision itself: which step needs evidence, which step needs judgment, which step can run unattended once governance is in place.
Microsoft's Work Trend Index data shows that knowledge workers in healthcare providers spend up to 30% of the week searching for or recreating information that already exists internally. Source-grounded retrieval is the highest-leverage AI use case in this segment.
Industry context: Mid-market and enterprise operators face the same fundamental tradeoff: AI must compress operational cycle time while remaining auditable and integrable with existing systems of record.
Benchmarks we hit
Reference benchmarks from production deployments of knowledge management in healthcare providers-comparable contexts. Sources noted per row. Your actuals are measured against the baseline captured in Discovery.
| Metric | Industry baseline | AI-native typical | Delta |
|---|---|---|---|
Source citation completeness Every claim grounded in approved source with replayable retrieval bundle | 38% | 100% | +62 pts |
Time-to-insight (analyst query → answer) Source-grounded retrieval + structured output; analyst validates rather than searches | 3.2 hours | 11 minutes | −94% |
Knowledge freshness (median age cited) Auto-refresh of approved sources + freshness scoring on retrieval | 94 days | 12 days | −87% |
Benchmarks are reference values from comparable engagements and authoritative sector benchmarks. Your engagement's baseline is captured during Discovery and actuals are reported weekly during Run against that baseline.
How we operate the workflow
Three commitments anchor how we run knowledge management in production for healthcare providers: every output is grounded in an approved source, every action is logged with the prompt and model version that produced it, every reviewer decision feeds the next iteration. Drop any one of the three and the workflow degrades within weeks — we have seen it happen, so we ship all three from week one.
What we build inside the workflow
Healthcare Providers workflows are bounded by the systems your team already uses. We do not propose a replacement of EHR; we build the AI-native operating layer on top of it. The Build engagement is fixed-price, scoped against the systems list captured in Discovery, and the integration footprint is part of the statement of work.
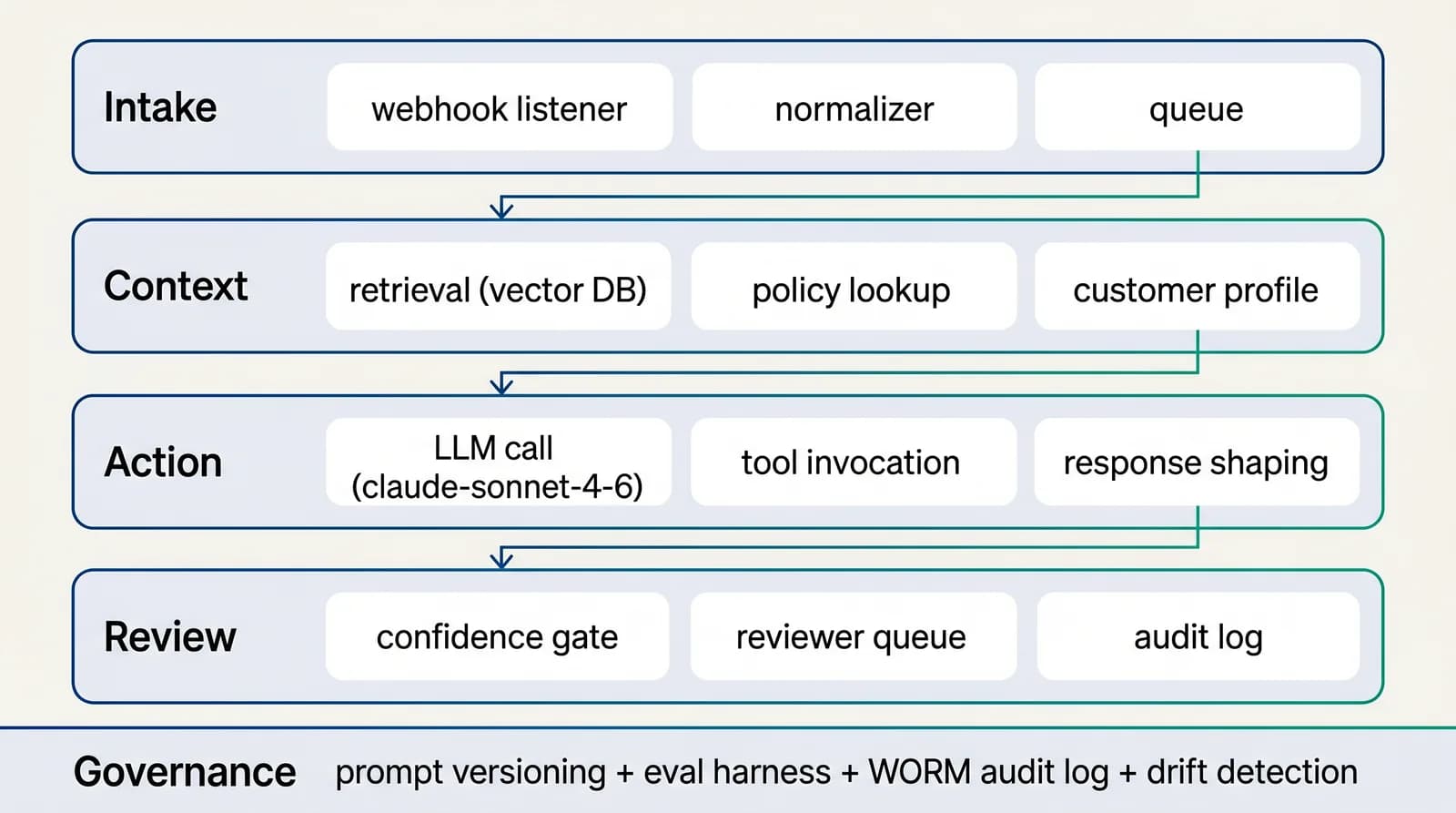
Reference architecture
4-layer AI-native workflow for knowledge & insight
Intake → context → action → review. The loop is closed: every reviewer decision feeds the next iteration of the prompt and the retrieval index. Without the closed loop, accuracy degrades silently over months.See the full architecture diagram for Knowledge & Insight →
AI-native vs traditional approach
How a scoped AI-native engagement compares to the alternatives for knowledge management in healthcare providers: in-house build, BPO retainer, generic SaaS subscription, traditional consulting engagement.
| Dimension | Traditional (in-house build or BPO) | AI-native engagement (us) |
|---|---|---|
| Time to production | Two quarters minimum | Production traffic within 6-10 weeks |
| Pricing model | FTE hourly retainer or fixed staffing | Three independent commercial envelopes |
| Audit / governance | Document-driven, periodic snapshot | Runtime guardrails + audit log + governance map + quarterly attestation |
| Operator throughput lift | 1.0× (baseline) | −94% |
| Cost per unit | Linear with operator headcount | Typically 60-80% lower |
| End-of-engagement | Multi-quarter notice + knowledge loss | Month-to-month Run, full handover plan in Build SoW |
Traditional process automation projects cost $80-200k+ with 6-12 month payback; AI-native engagements deliver thin-slice production in 6-8 weeks with measurable baseline-vs-actuals reporting.
Engagement scope & pricing
We run this as a fixed-scope engagement with a clear commercial envelope, not an open-ended retainer.
Insight engagement
Three phases, billed separately. You commit one phase at a time.
Phase 1 · Discovery
$6k
2-week sprint
Phase 2 · Build
$22k–$30k
7-10 weeks
Phase 3 · Run
$3k–$5k / mo
optional, hourly bank also available
~$34k–$60k typical year 1 (60% take the run option for ~6 months)
Source curation, retrieval architecture, evaluation harness, and decision dashboards.
Two-week Discovery, then your decision. Build is fixed-price against the Discovery output. Run, if you opt in, is month-to-month with a documented exit path.
The 4-phase delivery model
Phase 1 · Weeks 1–2
Discovery
We map the workflow, the systems, the decisions, and the baseline metrics. Output: a scoped statement of work.
Phase 2 · Weeks 2–4
Design
Two weeks of design produces the technical artefacts Build executes against: the workflow blueprint, the data-access plan, the prompt strategy, the review-queue UX, the audit-log shape, the dashboard wireframes.
Phase 3 · Weeks 4–8
Build
6-10 week sprint that ships the thin-slice production workflow on top of your existing systems. Eval harness gating every prompt change. Reviewer queue staffed. Audit log queryable. Dashboard live.
Phase 4 · Weeks 8+
Run
Run cadence is calibrated to your operational reality: weekly metric review, bi-weekly prompt refresh, monthly calibration audit, quarterly architecture review. The Run phase compounds value as the labelled test set grows.
Interactive ROI calculator
Estimate your AI-native ROI for knowledge management
Reference inputs below are typical for healthcare providers teams in the knowledge insight cluster. Adjust them to match your situation.
Projected
Current monthly cost
$26,400
AI-native monthly cost
$6,684
Annual savings
$236,592
75% cost reduction · ~1,672 operator-hours freed / month
Governance and risk controls
For healthcare providers teams operating under patient safety, clinical validation, privacy, consent, and equity, the governance stack we ship is opinionated: source allow-lists curated by your subject-matter expert, prompt versioning gated by your evaluation harness, reviewer queues staffed by your team, audit logs retained per your data policy. We bring the architecture; you bring the policy. The combination is what auditors recognize as defensible.
How we report ROI
The ROI metric that matters most for healthcare providers leadership on knowledge management is not labor savings — it is opportunity capture. Faster search success means more cases handled in the same window, more revenue, more compliance coverage, more customer trust. We measure both: the costs that drop and the throughput that scales.
Selected portfolio
Real builds — knowledge management in healthcare providers and adjacent sectors
Below are engagements drawn from our active portfolio where the workflow rhymed with knowledge management in healthcare providers or in adjacent contexts. Scope and stack are accurate; client identities are withheld under engagement NDAs.
Q3 2025
Radiology workflow application — case handling and reporting
Medical imaging operator · Europe
Application supporting radiology workflow: case intake, structured reporting, document handling, and quality-assurance loop. Designed for regulated medical-imaging context with audit trail and role-based access.
- Web app + secure storage
- Structured reporting
- Audit-trail compliance
Q1 2026
Premium bilingual corporate site + internal CRM
Multi-vertical consulting group · Europe
Corporate marketing site with animated bento-grid editorial, bilingual content architecture, and an internal CRM behind the scenes for lead handling. Designed to project a premium positioning aligned with enterprise buyers while keeping marketing-team ownership of the content layer.
- Next.js + animated bento grids
- Bilingual content layer
- Internal CRM integration
Q4 2025
Internal automation tool — workflow automation for consulting operations
Multi-vertical consulting group · Europe
Internal automation tool to streamline workflows, reduce manual administrative load, and improve operational efficiency across consulting and management processes. Integrates with existing systems rather than replacing them, automating handoffs and document flows that previously moved through email.
- Workflow automation engine
- Document-flow integration
- Operational dashboards
Client identities withheld under engagement NDAs. Sector, geography, and scope are accurate. Full case studies on request.
Common pitfall & mitigation
The failure mode we see most often on AI-native knowledge management engagements in healthcare providers contexts.
Decision dashboards become wallpaper
Beautiful dashboards, no action; the metric moved but nobody noticed
Alerting on metric movement + named owner per metric + weekly action review in Run
How the regulatory frame shapes the architecture
Three regulatory pressures shape every healthcare providers engagement we run on knowledge management. The first is explainability — the regulator's right to receive a coherent rationale for any decision the workflow produced, in language a senior examiner understands. The second is replayability — the ability to reconstruct the inputs, model versions, and reasoning chain that led to that decision, six months or two years later. The third is segregation of duties — the line between automated action, drafted-with-review, and reserved-to-human steps, with no operator able to silently widen the automation envelope.
We address all three at the architecture level rather than as policy overlays. Explainability is wired into the prompt pipeline: every customer-facing output ships with the supporting source citations, the confidence band, and the policy clauses the model applied. Replayability is wired into the audit log: every inference call is stored with its full input context, model fingerprint, retrieval bundle, and downstream effects, with a retention policy aligned to the regulator's longest plausible review window. Segregation is wired into the reviewer UI: each step has a typed permission, each escalation has a named owner, each policy-edit action requires a second pair of eyes from a different team.
The practical effect for healthcare providers leadership is that examinations stop feeling like archaeological digs. The supervisory question — "show me how this decision was made on date X" — becomes a one-query lookup in the audit log, returning the policy clauses, the source citations, the model version, the reviewer trail, and the downstream actions. The traditional posture would assemble that record over weeks; the AI-native posture assembles it on demand. That is the operational difference between a controlled AI workflow and a research prototype dressed in compliance language.
Data residency and sovereignty constraints in healthcare providers are easier to honor when designed into the architecture than when bolted on later. The retrieval index lives in your cloud region; the model provider is selected to align with your data-residency expectations; the audit log retention follows your jurisdiction's longest plausible review window. These are Discovery-phase decisions, not late-Build pivots, because reversing them costs months.
The concrete first-30-day delivery plan
Most healthcare providers AI projects fail in the first month for the same reason: too much time in scoping, too little in shipping. Our Build phase inverts that ratio deliberately. Week 1 has running code; week 4 has reviewable thin-slice production traffic; week 6 has a defensible accuracy baseline against the labelled test set.
The shape of the first week is opinionated. By end of day Wednesday, the retrieval index is loaded with the first batch of approved sources. By end of day Friday, the intake classifier is hitting the labelled test set with an initial accuracy number. The number is intentionally not impressive — it is a baseline against which weeks 2 and 3 measure progress. Most teams underestimate how motivating that early concrete number is for both the operator team (it stops feeling abstract) and the engineering team (the eval feedback loop is closing).
From week 2 onward the cadence is metric-driven. Every Friday produces a delta report against the labelled test set: which slices improved, which regressed, what the next iteration targets. The operator team participates in the Friday review; their judgment on edge cases becomes the next iteration's prompt or retrieval tweak. By week 6, the system has been through 12-15 evaluation cycles, each with healthcare providers-specific calibration, each tied to a documented change. The workflow that hits production at the end of Build is the workflow that has survived a month of empirical correction, not the workflow that looked good in the architecture diagram.
Closest precedent in our portfolio
The engagement that most closely rhymes with knowledge management in healthcare providers is summarised below. Identity withheld under engagement NDA; sector and stack are accurate.
Radiology workflow application — case handling and reporting. Application supporting radiology workflow: case intake, structured reporting, document handling, and quality-assurance loop. Designed for regulated medical-imaging context with audit trail and role-based access. (Medical imaging operator · Europe, Q3 2025.)
The architectural choices that worked there translate to healthcare providers knowledge management with two adjustments: the data-source mix shifts to match your operating systems (EHR, RCM, and adjacent), and the reviewer SLAs adjust to your team's operating cadence. The four-layer pattern (intake, context, action, review), the evaluation discipline, and the audit posture are portable.
For US buyers
US compliance scaffolding for knowledge management in healthcare providers (HIPAA, PHI, NIST AI RMF)
Healthcare Providers engagements touching US clients on knowledge management ship with the regulatory scaffolding your procurement, compliance, and legal teams expect. The framework that matters most for healthcare providers is Health Insurance Portability and Accountability Act (HIPAA) — addressed below alongside the adjacent frames we encounter.
HIPAA
Health Insurance Portability and Accountability Act
Authority: U.S. Department of Health and Human Services / OCR
- Scope
- Protected Health Information (PHI) handling, security safeguards, breach notification, business associate accountability.
- How we ship inside it
- We sign a Business Associate Agreement (BAA) on healthcare engagements that touch PHI. The architecture supports BAA-covered model providers (Anthropic BAA, Azure OpenAI BAA, AWS Bedrock BAA). Audit log retention defaults to 6 years (HIPAA minimum). PHI handling follows minimum-necessary principle at the prompt and retrieval layers.
PHI
Protected Health Information
Authority: HIPAA Privacy Rule
- Scope
- Any health information that can identify an individual.
- How we ship inside it
- PHI is redacted before transmission to non-BAA model providers; retention follows BAA terms; access is logged at the user level. Workflows touching PHI are deployed to BAA-covered infrastructure only.
NIST AI RMF
NIST AI Risk Management Framework (AI 100-1)
Authority: U.S. National Institute of Standards and Technology
- Scope
- Voluntary framework: Govern, Map, Measure, Manage functions for AI system risk.
- How we ship inside it
- Every engagement maps to NIST AI RMF during Discovery. The control map produced becomes the artefact your internal audit and security teams use to defend the workflow.
For US companies
Start a US-friendly engagement
Discovery from $8,500–$12,000, Build from $35,000–$75,000, optional Run from $5k/mo. Fixed-price, milestone-billed, you own every artefact. Send a short brief and we reply within 5 business days. 11am–4pm ET overlap for live syncs.
USD pricing
Discovery $8,500–$12,000 · Build $35,000–$75,000
US-style commercial
MSA / SOW / mutual NDA standard. DPA with SCCs included.
Limited capacity
We onboard 3–5 new clients per quarter to protect delivery quality.
Build internally or work with us
The opportunity cost of building first in healthcare providers is often invisible: 6-9 months spent hiring, tooling, and converging on a reference architecture is 6-9 months of competitors shipping. The engagement model we propose front-loads the reference architecture and the senior delivery team, then transitions the operation to your team once the pattern is proven.
What to ask us before signing
- Ask for a workflow map that shows intake, retrieval, generation, review, escalation, system updates, and measurement.
- Ask for an evaluation plan using real examples from healthcare providers, not only generic test prompts.
- Ask how we will move search success, time saved, knowledge freshness, and repeated question reduction within the first 30 to 60 days.
- Ask which parts of the process remain human-owned and why.
- Ask for our exit plan: what stays with you if the engagement ends.
Recommended first project
If you can pick only one wedge, pick the knowledge management subflow that is currently absorbing the most senior-operator time on cases that are mostly routine but require context the system does not surface today. That subflow has the highest immediate ROI and the cleanest path to a labelled test set. We have shipped this pattern across enough healthcare providers engagements to know which subflows compound and which stall. The Discovery sprint identifies the wedge concretely. The Build phase ships it as a thin slice within 6-8 weeks. The Run phase compounds value as the labelled test set grows, the prompt library tunes to your category, and the reviewer team calibrates against real traffic. The 90-day milestone is a defensible empirical track record on which to scope the next engagement.
Frequently asked questions
How do you automate knowledge management in healthcare providers with AI?+
Three phases. Discovery (2 weeks) produces the labelled test set, the system map, and the Build statement of work. Build (6-10 weeks) ships a thin-slice production deployment on top of EHR and adjacent systems, with versioned prompts and a reviewer queue. Run (optional, month-to-month) operates the workflow weekly against search success, time saved, knowledge freshness, and repeated question reduction.
What does it cost to automate knowledge management for healthcare providers teams?+
Three phases, billed separately. Discovery sprint: $6k (2-week sprint). Build engagement: $22k–$30k (7-10 weeks). Run retainer: $3k–$5k / mo (optional, hourly bank also available). ~$34k–$60k typical year 1 (60% take the run option for ~6 months). Source curation, retrieval architecture, evaluation harness, and decision dashboards.
What is the best AI agent for knowledge management in healthcare providers?+
There is no single "best" off-the-shelf agent for knowledge management in healthcare providers — the right architecture depends on your EHR setup, your data, and your risk profile. We typically combine a frontier LLM (Claude, GPT-4-class, or Gemini) with a retrieval layer over your approved sources, tool-use for EHR and RCM integrations, and a reviewer queue. We benchmark candidate models against a labelled test set during Discovery and pick the one with the best accuracy/cost ratio for your workflow.
How long does it take to deploy AI knowledge management for healthcare providers?+
End-to-end lead time from kickoff to thin-slice production: 6-10 weeks. End-to-end to full operating envelope: 10-14 weeks. search success, time saved, knowledge freshness, and repeated question reduction is instrumented from day one of Build; the dashboard goes live by week 4-5; production traffic starts by week 6-8. By 90 days, leadership has a 30-60 day record of operating performance against the Discovery baseline.
What do we own, and what do you own?+
We own the workflow design, the prompts, the retrieval architecture, the evaluation harness, and weekly improvement. Your hospital systems, clinics, care operations leaders, and patient access teams team owns data access, policy, exception approval, and final commercial decisions. At the end of the engagement, every prompt, eval, and config is handed over — no lock-in.
How do you prevent hallucination on consequential answers?+
Grounded retrieval is non-negotiable — every claim in a generated answer must trace to a citation in the approved source corpus. The retrieval layer is curated by a subject-matter expert from your team, refreshed on a documented cadence, and audited quarterly. Anything below a confidence threshold routes to a reviewer with the supporting evidence pre-assembled.
Do you train models on our data?+
No. We do not train any model on client data. Anthropic Zero-Data-Retention is enabled by default; OpenAI default-no-training is honoured. Prompts, retrieval indexes, audit logs, and integration data live in your cloud account under your IAM. At engagement end, every artefact transfers to your repository.
What if we want to exit the engagement?+
Discovery and Build are fixed-scope, so there is no mid-engagement exit cost. Run is month-to-month with 30-day notice. Every artefact (prompts, eval harness, integration code, dashboards, runbooks) is in your repository throughout the engagement, not behind our SaaS. There is no lock-in.
What does success look like 90 days after Build closes?+
search success, time saved, knowledge freshness, and repeated question reduction measurably improved against the Discovery baseline. Your team is operating the workflow with the cadence we shipped during Build. The audit log is queryable. The reviewer queue is calibrated. The next workflow scope is informed by real production evidence rather than initial assumptions.
What support is included after the engagement ends?+
Optional Run retainer covers weekly cadence, prompt refresh, retrieval index updates, and reviewer-queue calibration. Architecture-level questions and breaking-change support are billed hourly outside of Run. Most engagements transition Run in-house at month 6-12; we stay available for architecture decisions for 12 months at no extra charge.
How does this integrate with EHR and our existing stack?+
Discovery scopes the integration footprint explicitly. We integrate at the API layer; no replatforming required. The Build statement of work names exactly which systems are connected, which data flows are bidirectional, and what authentication patterns we use (SSO, service accounts, OAuth scopes). The integration code lives in your repository.
What does your team look like during an engagement?+
Discovery: 1 senior delivery lead + 1 PM, ~30 hours/week. Build: 1 senior delivery lead + 2-3 senior AI engineers, ~50-80 hours/week across the team. Run: 1 delivery owner + 1 engineer on weekly cadence. We do not use offshore staff augmentation. Every engineer touching your engagement is senior-level.
Sources we reference
The following sources inform the architecture, governance, and benchmarks we apply on healthcare providers engagements. Cited here so you can verify and dig deeper.
- WHO Artificial Intelligence for Health
- AI Adoption Statistics — U.S. Bureau of Labor Statistics
- AI Risk Management Framework (AI RMF 1.0) — NIST
- Retrieval-Augmented Generation for Knowledge-Intensive NLP Tasks — Lewis et al., Meta AI Research
- Lost in the Middle: How Language Models Use Long Contexts — Liu et al., Stanford
- Google Search Central: helpful, reliable, people-first content
- Google Search Central: URL structure best practices
High-intent reads
Start the engagement
Start a Healthcare Providers engagement
Tell us about your workflow, the systems involved, and the KPI you want to move. We'll send a scoped statement of work within 5 business days.