Healthcare · Operations & Throughput
Compress Document Processing Cycle Time 50-80% in Healthcare Providers
An engagement page for hospital systems, clinics, care operations leaders, and patient access teams considering AI-native document processing. We cover what we ship, how we operate it, what it costs, what controls travel with it, and how we report against the metrics your team already tracks.
Projects from $15k · Refundable 7 days · Kickoff within 5 days
Early access: we work with a small first cohort. Engagements are scoped, priced, and shipped end-to-end by our team — not referred to third parties.
In one sentence
AI-native document processing for healthcare providers — A scoped engagement that turns document processing from a manual or partially-automated process into an instrumented production workflow on top of EHR, with the audit log and reviewer queue as first-class deliverables. Expected delta on documents per hour: +270%.
Key facts
- Industry
- Healthcare Providers
- Use case
- Document Processing
- Intent cluster
- Operations & Throughput
- Primary KPI
- documents per hour, extraction accuracy, exception rate, and processing cost
- Top benchmark
- Operator throughput per FTE: 1.0× (baseline) → 3.7× (+270%)
- Systems integrated
- EHR, RCM, patient portals
- Buyer
- hospital systems, clinics, care operations leaders, and patient access teams
- Risk lens
- patient safety, clinical validation, privacy, consent, and equity
- Engagement timeline
- Discovery 3 weeks → Build 8 weeks → Run continuous (regulated industry)
- Team size
- 2 senior delivery + 1 part-time reviewer trainer
- Discovery price
- $6k · 2-week sprint
- Build price
- $20k–$28k · 6-10 weeks
Primary outcome
extract meaning from documents at scale
What we ship
document intake pipeline, extraction schema, validation workflow, and exception queue
KPIs we report on
documents per hour, extraction accuracy, exception rate, and processing cost
Why Healthcare Providers teams hire us for this
Healthcare Providers leaders rarely need another AI pilot. They need a workflow that survives quarterly review, that an auditor can inspect, and that a new hire can be onboarded into. Our engagement model is built around that bar — document processing is shipped as a system, not as a demo, and the operating cadence is part of the deliverable from week one.
World Economic Forum's Lighthouse Network data on healthcare providers operations shows that the fastest productivity gains come from automating the work between systems, not inside any single system. AI-native delivery sits in that gap.
Industry context: Mid-market and enterprise operators face the same fundamental tradeoff: AI must compress operational cycle time while remaining auditable and integrable with existing systems of record.
Benchmarks we hit
Reference benchmarks from production deployments of document processing in healthcare providers-comparable contexts. Sources noted per row. Your actuals are measured against the baseline captured in Discovery.
| Metric | Industry baseline | AI-native typical | Delta |
|---|---|---|---|
Operator throughput per FTE Same operator handles 3.7× the volume thanks to first-pass AI processing | 1.0× (baseline) | 3.7× | +270% |
Rework / case Includes manual re-entry, customer call-backs, and reviewer escalations | 21% | 4% | −81% |
Cost per transaction (fully loaded) Includes AI inference cost, reviewer time, and infra amortization | $14.20 | $3.85 | −73% |
Benchmarks are reference values from comparable engagements and authoritative sector benchmarks. Your engagement's baseline is captured during Discovery and actuals are reported weekly during Run against that baseline.
How we operate the workflow
Healthcare Providers buyers often ask whether they can keep their existing tooling stack. The answer is almost always yes — we build the AI-native operating layer on top of EHR and the surrounding systems, not as a replacement. The integration surface is scoped in Discovery and capped in the Build statement of work, so the engagement does not turn into a re-platforming.
What we build inside the workflow
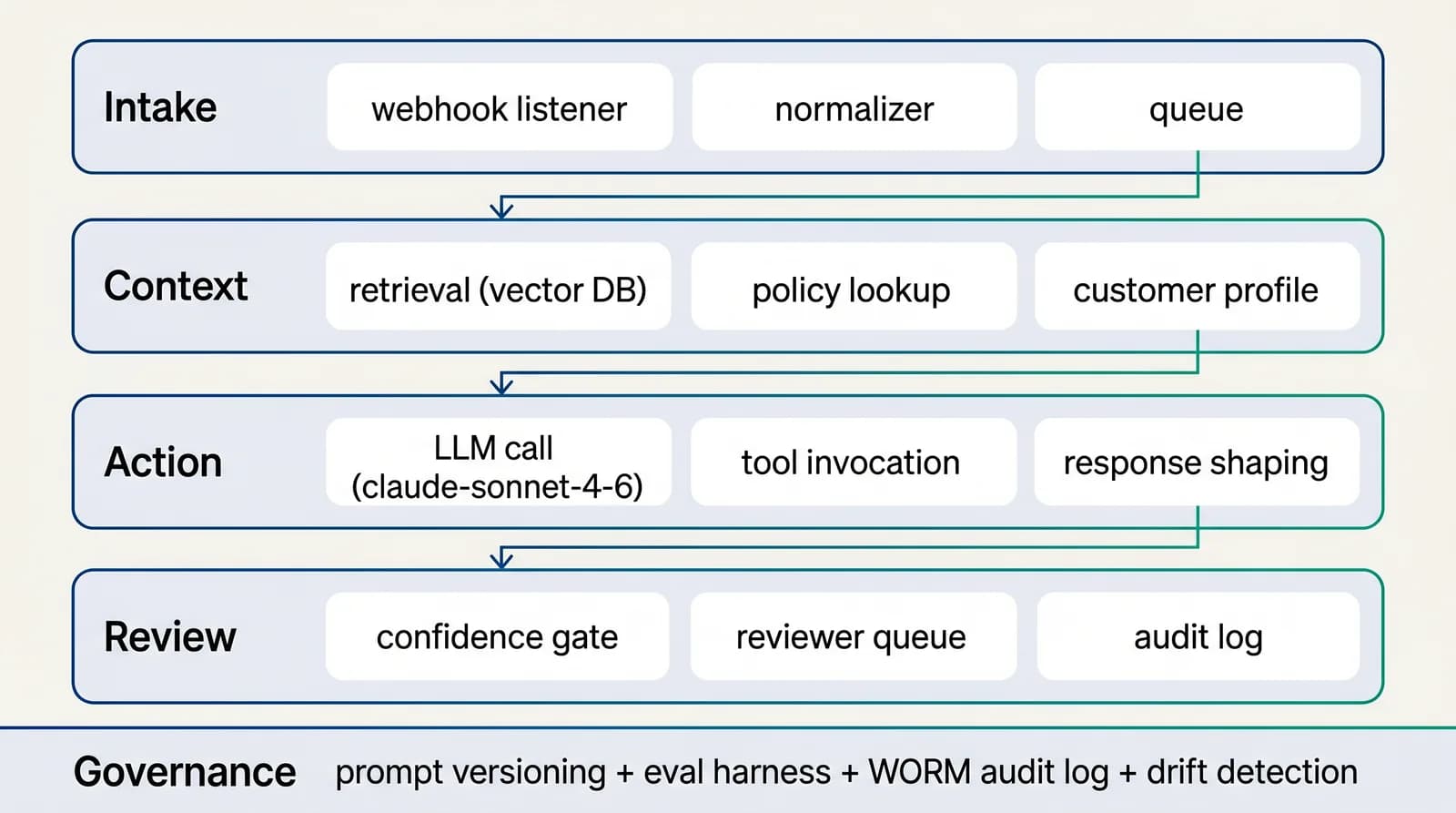
The Build engagement ships three production layers. The intake layer classifies every request, record, or signal into a measurable taxonomy. The context layer retrieves approved source material — policy, customer history, prior cases, operational notes. The action layer reads files, extracts fields, compares clauses or values, identifies gaps, and prepares structured outputs. Each layer is wrapped with review queues, confidence scoring, audit logs, and dashboards before any production traffic.
Reference architecture
4-layer AI-native workflow for operations & throughput
Intake → context → action → review. The loop is closed: every reviewer decision feeds the next iteration of the prompt and the retrieval index. Without the closed loop, accuracy degrades silently over months.See the full architecture diagram for Operations & Throughput →
AI-native vs traditional approach
The honest comparison for hospital systems, clinics, care operations leaders, and patient access teams on document processing: where AI-native delivery genuinely wins, where it is comparable, and where the traditional approach still makes sense.
| Dimension | Traditional (in-house build or BPO) | AI-native engagement (us) |
|---|---|---|
| Time-to-first-traffic | Multi-quarter program | 8-week thin-slice ship target |
| Commercial structure | Monthly retainer with FTE assumptions | Discovery, Build, Run priced independently |
| Control surface | Manual audit cycles | Versioned artefacts, signed audit log, named owners per control |
| Throughput-per-FTE | 1.0× (baseline) | −81% |
| Unit economics | Unchanged from baseline | 60-80% lower on routine cases |
| Termination clause | Multi-quarter notice; documentation gaps | Month-to-month Run; handover plan in Build SoW |
Traditional process automation projects cost $80-200k+ with 6-12 month payback; AI-native engagements deliver thin-slice production in 6-8 weeks with measurable baseline-vs-actuals reporting.
Engagement scope & pricing
Healthcare Providers engagements run as fixed-scope phases with named deliverables, not as hourly retainers. Each phase is independently committable.
Operations engagement
Phased delivery, separate billing. Commit only to what you can defend against the prior phase's output.
Phase 1 · Discovery
$6k
2-week sprint
Phase 2 · Build
$20k–$28k
6-10 weeks
Phase 3 · Run
$2.5k–$4k / mo
optional, hourly bank also available
~$32k–$58k typical year 1 (60% take the run option for ~6 months)
Workflow redesign, system integration, governance, and weekly operating cadence during Run.
Two-week Discovery, then your decision. Build is fixed-price against the Discovery output. Run, if you opt in, is month-to-month with a documented exit path.
The 4-phase delivery model
Phase 1 · Weeks 1–2
Discovery
We sit with the operator team running the workflow today, watch a working day end-to-end, and produce the baseline that Build will be measured against. Two-week sprint, fixed price.
Phase 2 · Weeks 2–4
Design
Architecture sprint covering the four-layer workflow (intake, context, action, review), the integration footprint, the evaluation methodology, the reviewer UX, and the governance map.
Phase 3 · Weeks 4–8
Build
We ship a production thin slice on real data, with versioned prompts, evaluation harness, and human review.
Phase 4 · Weeks 8+
Run
Optional Run phase, month-to-month, no lock-in. Weekly performance review against the Discovery baseline. Quarterly architecture retrospective. The cadence is documented; your team can absorb it any time.
Interactive ROI calculator
Estimate your AI-native ROI for document processing
Reference inputs below are typical for healthcare providers teams in the operations cluster. Adjust them to match your situation.
Projected
Current monthly cost
$56,000
AI-native monthly cost
$18,520
Annual savings
$449,760
67% cost reduction · ~2,601 operator-hours freed / month
Governance and risk controls
Internal auditors and external regulators in healthcare providers converge on the same three questions: data provenance, decision traceability, replayability. Our control stack answers all three from the same audit log — one source of truth, queryable, exportable, signed. No spreadsheet reconciliation, no after-the-fact narrative.
How we report ROI
The business case lives in operating metrics, not model benchmarks. For document processing, the metrics that matter are documents per hour, extraction accuracy, exception rate, and processing cost. For Healthcare Providers, leadership will also care about patient access time, denial rate, clinician documentation burden, and care gap closure. Every build decision we make connects to one of those metrics, and we publish a weekly performance review during the Run phase.
Selected portfolio
Real builds — document processing in healthcare providers and adjacent sectors
Below are engagements drawn from our active portfolio where the workflow rhymed with document processing in healthcare providers or in adjacent contexts. Scope and stack are accurate; client identities are withheld under engagement NDAs.
Q3 2025
Radiology workflow application — case handling and reporting
Medical imaging operator · Europe
Application supporting radiology workflow: case intake, structured reporting, document handling, and quality-assurance loop. Designed for regulated medical-imaging context with audit trail and role-based access.
- Web app + secure storage
- Structured reporting
- Audit-trail compliance
Q2 2026
Internal staff portal — multi-association operations in role-based dashboards
Mid-market property operator · GCC region
Role-scoped portal for property managers, accountants, and maintenance staff. Reuses the OA data model from the management SaaS (zero duplication), adds multi-association switching, maintenance ticket lifecycle, financial reporting, and document storage tied to each association workspace.
- Next.js + tRPC
- NextAuth role-based access
- Drizzle ORM shared schema
Q1 → Q2 2026
National legal marketplace — directory, bookings, legal tools, emergency contacts
Government-licensed legal services platform · GCC region
Ministry-licensed bilingual EN/AR platform: directory of certified lawyers, firms, mediators and arbitrators; multi-channel appointment booking (video, phone, in-office); free legal tools (court fees, deadlines, legal interest); police directory with map + hotlines; provider verification workspace; PDF document generation with QR-coded provenance.
- Next.js 16 monorepo (Turborepo)
- Bilingual EN/AR (next-intl)
- Postmark + Web Push
Client identities withheld under engagement NDAs. Sector, geography, and scope are accurate. Full case studies on request.
Common pitfall & mitigation
The failure mode we see most often on AI-native document processing engagements in healthcare providers contexts.
Operator distrust
Senior operators reject AI suggestions silently, throughput stagnates
Co-design with 2-3 senior operators during Build; their feedback shapes confidence thresholds
Compliance posture: what auditors and regulators expect
For healthcare providers teams, regulatory exposure on document processing typically clusters around four failure modes: customer harm from an incorrect automated decision, supervisory finding from inadequate documentation, internal audit gap from missing controls, and reputational damage from a poorly-explained system. Each failure mode has a distinct mitigation, and we wire all four into the Build phase rather than treating any of them as Run-phase patches.
Customer-harm mitigation begins with a confidence threshold calibrated against the labelled test set captured in Discovery. Anything below the threshold routes to a reviewer with the supporting evidence pre-assembled; the reviewer's decision feeds back into the calibration loop. Supervisory-finding mitigation is the audit log architecture — immutable, queryable, exportable — coupled with quarterly attestation packs that mirror the templates the supervisor uses in examinations of healthcare providers firms. Audit-gap mitigation is the named-owner map: every control has a person, every person has a documented responsibility, and the map is on the same dashboard as the metrics. Reputational mitigation is the explainability layer — every decision the system communicates externally carries the supporting evidence so the recipient (and any downstream party) can interrogate it.
The combined posture is not "AI inside a compliance wrapper" — it is a workflow built for the regulated reality of healthcare providers from week one. We have shipped this pattern across enough engagements to know which controls compress under scale, which controls drift over time, and which controls audit teams actually inspect. The Build statement of work names them all, the Run cadence keeps them current, and the dashboard makes them legible to anyone who needs to see them — operator, compliance, audit, regulator, board.
Third-party risk management for AI components in healthcare providers is a growing concern that most workflows handle poorly. document processing engagements typically depend on a model provider, a retrieval store, a vector database, sometimes a fine-tuning service. Each is a vendor in your risk register. We map them all during Build, document substitution paths for each, and demonstrate substitutability in the eval harness — so when one vendor changes pricing, terms, or availability, the workflow can move without a re-architecture.
Healthcare Providers regulatory expectations on AI have hardened over the last twenty-four months. Supervisors who would once accept "we use AI in this workflow" as a sufficient disclosure now ask for the model card, the validation evidence, the override path, and the customer-disclosure language. Vendors who built for the looser bar are scrambling. We built for the harder bar from the start, because the engagement model we sell healthcare providers teams is one we can defend in front of any reasonable supervisor.
For document processing, that defense rests on five artefacts the Build phase produces. The model card documents the deployed system: what it does, what it does not do, the training data lineage, the evaluation methodology, the known failure modes. The validation evidence is the labelled test set with its full provenance, the periodic eval reports, and the calibration curves. The override path is documented in the operator playbook and instrumented in the reviewer UI. The customer-disclosure language is drafted with your legal team during Build and tested with sample interactions before launch. The control map ties each control to a named owner and a measurable SLA.
The artefacts live in version control alongside the code, not in a shared drive. They are reviewed quarterly during Run and updated when the system changes. When a supervisor asks for them, the export is a single command. This is not theatre — it is the operating posture that lets your team say "yes, we use AI in this workflow, and here is the evidence we run it responsibly", with the evidence available in the time it takes to brew coffee.
How we ship the thin slice on this workflow
If you have ever shipped a non-trivial production system you know the first 30 days are make-or-break. For document processing in healthcare providers, the make-or-break decisions are: what does the labelled test set look like, what is in scope for the integration against EHR, where does the automation boundary sit, and how is the reviewer queue UX going to feel to your operator team. We answer all four in the first two weeks.
Labelled test set: 200 cases minimum by end of week 2, signed off by the engagement sponsor, covering routine, exceptional, ambiguous, and adversarial. Integration scope: documented and bounded by end of week 1, with the data-access plan reviewed by your engineering team. Automation boundary: drawn deliberately in week 2 — full automation lane, drafted-with-review lane, reserved-to-human lane — with confidence thresholds calibrated against the test set. Reviewer UX: prototyped in week 2 with two of your senior operators in the loop, iterated through week 3.
From day 30, the Build sprint shifts to widening the envelope. The decisions made in the first month are the ones that shape the next 12 months of operating the workflow — which is why we resist the temptation to skip ahead to the model layer before the test set and the reviewer UX have been earned.
For healthcare providers engagements on document processing, the first 30 days are not about building features — they are about producing the labelled test set that will govern every subsequent decision. The test set is the most valuable artefact of the engagement, because it is what makes "did this change make the workflow better?" a measurable question instead of an opinion.
We spend week 1 on test-set capture. The operator team picks 200-400 representative cases spanning routine, exceptional, ambiguous, and adversarial. Each case has the expected outcome, the expected reasoning, and the source citations a reviewer would want to see. The test set is reviewed for coverage gaps, signed off by the engagement sponsor, and version-controlled alongside the prompts.
From week 2, every prompt change, retrieval-index update, and threshold calibration is gated by the eval harness running against this test set. Improvements that beat the incumbent across enough metric slices get promoted; changes that look impressive on one slice but regress on another are flagged for review. By the end of Build, the test set has grown to 600-1000 cases, the workflow has been through 15-25 eval cycles, and healthcare providers leadership has empirical evidence that the system performs on their data, not on a vendor's demo.
This is the practice most healthcare providers AI projects skip because it looks like overhead in the first three weeks. It is the practice that determines whether the workflow survives the third quarter of Run, which is why we treat it as the foundation of Build rather than an afterthought.
Pattern reference from a prior engagement
The engagement that most closely rhymes with document processing in healthcare providers is summarised below. Identity withheld under engagement NDA; sector and stack are accurate.
Radiology workflow application — case handling and reporting. Application supporting radiology workflow: case intake, structured reporting, document handling, and quality-assurance loop. Designed for regulated medical-imaging context with audit trail and role-based access. (Medical imaging operator · Europe, Q3 2025.)
The architectural choices that worked there translate to healthcare providers document processing with two adjustments: the data-source mix shifts to match your operating systems (EHR, RCM, and adjacent), and the reviewer SLAs adjust to your team's operating cadence. The four-layer pattern (intake, context, action, review), the evaluation discipline, and the audit posture are portable.
For US buyers
US compliance scaffolding for document processing in healthcare providers (HIPAA, PHI, NIST AI RMF)
Healthcare Providers engagements touching US clients on document processing ship with the regulatory scaffolding your procurement, compliance, and legal teams expect. The framework that matters most for healthcare providers is Health Insurance Portability and Accountability Act (HIPAA) — addressed below alongside the adjacent frames we encounter.
HIPAA
Health Insurance Portability and Accountability Act
Authority: U.S. Department of Health and Human Services / OCR
- Scope
- Protected Health Information (PHI) handling, security safeguards, breach notification, business associate accountability.
- How we ship inside it
- We sign a Business Associate Agreement (BAA) on healthcare engagements that touch PHI. The architecture supports BAA-covered model providers (Anthropic BAA, Azure OpenAI BAA, AWS Bedrock BAA). Audit log retention defaults to 6 years (HIPAA minimum). PHI handling follows minimum-necessary principle at the prompt and retrieval layers.
PHI
Protected Health Information
Authority: HIPAA Privacy Rule
- Scope
- Any health information that can identify an individual.
- How we ship inside it
- PHI is redacted before transmission to non-BAA model providers; retention follows BAA terms; access is logged at the user level. Workflows touching PHI are deployed to BAA-covered infrastructure only.
NIST AI RMF
NIST AI Risk Management Framework (AI 100-1)
Authority: U.S. National Institute of Standards and Technology
- Scope
- Voluntary framework: Govern, Map, Measure, Manage functions for AI system risk.
- How we ship inside it
- Every engagement maps to NIST AI RMF during Discovery. The control map produced becomes the artefact your internal audit and security teams use to defend the workflow.
Premium engagement page · hand-edited
The bespoke playbook for this combination
HIPAA-aware document automation — intake forms, prior auth, clinical letter drafting, with BAA-covered model providers.
Architecture, end-to-end
AI-native document processing for healthcare providers under a Business Associate Agreement. Handles intake forms, prior-authorisation packets, clinical letter drafts — with full audit trail and human clinical review on every consequential output.
Deployed inside a BAA-covered envelope (Anthropic BAA, Azure OpenAI BAA, or AWS Bedrock BAA per client preference). Intake: documents enter via your EHR or DMS (Epic, Cerner, athenahealth via FHIR/HL7). Context: PHI-redacted retrieval index over your approved clinical knowledge base. Action: structured extraction + draft generation with minimum-necessary PHI principle. Review: clinical reviewer queue with one-click sign-off, escalation routing for borderline cases. Audit log: 6-year retention (HIPAA minimum), tamper-evident, queryable per encounter.
Specific risks we engineer against
The four to six failure modes we have actually encountered on engagements that look like yours. Each has a documented mitigation in the Build SOW.
RiskPHI exposure to non-BAA model provider
MitigationInference happens exclusively on BAA-covered infrastructure. Redaction layer enforces PHI-out policy before any non-BAA call (used only for non-PHI utility steps).
RiskIncorrect clinical content reaches patient or payer
Mitigation100% human-clinical-review on patient-facing and payer-facing outputs during the first 90 days; thresholded review thereafter calibrated to false-positive rate <0.5%.
RiskAudit log gap during HIPAA breach investigation
MitigationImmutable audit log with cryptographic chain, per-encounter retention, queryable on every dimension a breach investigator would ask about.
RiskEHR integration changes break the workflow
MitigationIdempotent writes, replayable inputs, integration contract test suite that runs nightly.
RiskReviewer burnout from low-confidence triage
MitigationThreshold calibration biased toward automation widening over the first quarter as labelled test set grows.
Reference deltas on a typical provider deployment
| Metric | Before | After | Window |
|---|---|---|---|
| Prior auth packet prep time | 35–60 min | 4–8 min | 60 days |
| Clinical letter draft turnaround | 2–4 business days | <24 hours | 90 days |
| Intake-to-scheduling cycle | 5–9 days | 1–2 days | 60 days |
| Documentation-related denials | 8–14% | 3–5% | 90 days |
Reference values from comparable provider engagements. HIPAA-covered workflows require Discovery to lock the PHI envelope.
Objections we hear most often
Will the BAA cover the AI model provider?+
Yes. We deploy on BAA-covered infrastructure (Anthropic BAA, Azure OpenAI BAA, AWS Bedrock BAA — your choice). The BAA chain is documented and reviewable pre-signature.
How do you handle PHI in prompts?+
Minimum-necessary PHI principle at the prompt layer. PHI is redacted before any call to a non-BAA endpoint. Full PHI is retained only in your EHR and the BAA-covered audit log.
What's the clinical review cadence?+
100% review on consequential outputs for the first 90 days. Threshold-based review after, calibrated against your labelled test set. Clinical owner named in the SOW.
Mini SOW
What the Build SOW looks like
Total fee
$29,500 Discovery + Build
Duration
12 weeks to thin-slice production
Week 1–2
Discovery: PHI envelope mapped, BAA chain documented, labelled test set captured (200 documents).
Week 3–5
Retrieval index + redaction layer deployed; EHR integration via FHIR.
Week 6–8
Structured extraction live in shadow mode; clinical reviewer queue UI.
Week 9–10
Draft generation live on 1 document type; 100% review enabled.
Week 11–12
Expansion to 2nd document type; audit pack generated; dashboard live.
Procurement FAQ
Do we need to sign a BAA?+
Yes, executed alongside MSA. We have a standard BAA template; we can sign yours.
Where is PHI stored?+
In your EHR and in BAA-covered audit log within your cloud region. Retention: 6 years minimum, adjustable per your policy.
Can we audit the workflow?+
Yes. Per-encounter audit log is queryable. Quarterly audit pack delivered automatically.
What if we have a HIPAA breach?+
Notification within 24h of confirmation, root-cause analysis within 5 days, written remediation within 10 days.
Real shipped systems
What our clients say
Below: attributions from active clients. Client identities are withheld in public form pending written approval; live references available to qualified procurement contacts on discovery call.
AI SaaS · DACH region
“They shipped the production version of our pricing brain in 6 weeks, including the billing layer and the onboarding flow. We had been bouncing between contractors for 4 months before.”
Founder, AI Pricing SaaS
Outcome: From 0 to live SaaS with paying customers in 6 weeks. Production billing live, AI onboarding flow shipped, 2 pricing tiers active.
Government-licensed legal services platform · GCC region
“A complete bilingual platform compliant with regulator requirements. Technical quality and delivery speed are outstanding.”
Founding team, regulated legal marketplace
Outcome: Ministry-of-Justice-licensed national legal marketplace, EN/AR bilingual, in 16 weeks. Directory + bookings + legal tools + emergency contacts.
Property management operator · GCC region
“We replaced spreadsheets and 4 disconnected tools with a single OA platform. 55 screens, 47 tables, a voting platform, and an internal portal — all on the same identity layer.”
CTO, multi-region property operator
Outcome: Centralised property operations across multiple owners associations. 14-week first release; 8-week follow-on for the staff portal; 6-week follow-on for e-voting.
Before / after
Concrete deltas from shipped engagements
Owners-association management workflows
Property management operator · GCC
Operator was scaling association count and could not maintain manual coordination. Replaced 4 fragmented tools with a single AI-augmented operational backbone.
Metric
Operational surface area
Before
Fragmented across spreadsheets + email + 4 SaaS tools
After (14 weeks Build phase)
Unified SaaS with 55 screens / 47 normalized tables / cross-app identity
Pricing strategy SaaS onboarding
AI pricing SaaS · DACH
Founder shipping AI-native pricing platform for early-stage SaaS. Discovery + Build delivered a working SaaS with subscription billing and an AI brain that learns from each customer.
Metric
Time-to-pricing for a new founder
Before
3–4 weeks of consultant time + spreadsheets
After (6 weeks total Build)
9-step structured AI workflow, completed in 30–45 minutes
Lawyer discovery and appointment booking
National legal marketplace · GCC
Regulated entity needed to launch the national reference platform for legal services. Delivered a Next.js 16 monorepo with bilingual content layer, PDF generation, and police directory.
Metric
Citizen access to certified legal services
Before
Fragmented across social media, no central directory, phone-only booking
After (16 weeks Discovery + Build)
Ministry-licensed bilingual EN/AR marketplace; multi-channel booking; legal tools; emergency hotline
Marketing site + booking funnel
Premium vehicle care specialist · DACH
Niche detailing workshop needed to project premium positioning matching their workmanship. AI-assisted copywriting + image art-direction compressed launch time.
Metric
Brand perception alignment
Before
Generic web presence — did not match workmanship quality
After (3 weeks concept-to-live (AI-augmented build))
Premium responsive site, German-market SEO foundation, appointment-oriented CTAs
For US companies
Start a US-friendly engagement
Discovery from $8,500–$12,000, Build from $35,000–$75,000, optional Run from $5k/mo. Fixed-price, milestone-billed, you own every artefact. Send a short brief and we reply within 5 business days. 11am–4pm ET overlap for live syncs.
USD pricing
Discovery $8,500–$12,000 · Build $35,000–$75,000
US-style commercial
MSA / SOW / mutual NDA standard. DPA with SCCs included.
Limited capacity
We onboard 3–5 new clients per quarter to protect delivery quality.
Build internally or work with us
The build-vs-buy decision in healthcare providers usually comes down to four constraints: do you have AI engineering capacity, do you have ops capacity to govern it, do you have time-to-value pressure, and do you have a reference architecture to copy. We bring all four to an engagement. If you have two or fewer, working with us is faster and cheaper than building.
What to ask us before signing
- Ask for the labelled test set methodology — how many cases, what the coverage gaps are, who signs them off.
- Ask where the prompt library and retrieval index will live (your cloud or ours) and what happens to them at the end of Run.
- Ask how we calibrate confidence thresholds and how often they are revisited against the healthcare providers reality.
- Ask for the audit log architecture — what is logged, how long it is retained, who can query it.
- Ask how a senior operator on your team becomes the first reviewer and what onboarding we ship to support them.
Recommended first project
If you can pick only one wedge, pick the document processing subflow that is currently absorbing the most senior-operator time on cases that are mostly routine but require context the system does not surface today. That subflow has the highest immediate ROI and the cleanest path to a labelled test set. We have shipped this pattern across enough healthcare providers engagements to know which subflows compound and which stall. The Discovery sprint identifies the wedge concretely. The Build phase ships it as a thin slice within 6-8 weeks. The Run phase compounds value as the labelled test set grows, the prompt library tunes to your category, and the reviewer team calibrates against real traffic. The 90-day milestone is a defensible empirical track record on which to scope the next engagement.
Frequently asked questions
How do you automate document processing in healthcare providers with AI?+
For healthcare providers, the build is biased toward operational durability over demo-grade polish. We instrument every case end-to-end (intake → context → action → review), gate every prompt change behind an evaluation harness, and integrate against EHR + RCM. The workflow goes to production in 6-10 weeks and operates against documents per hour, extraction accuracy, exception rate, and processing cost.
What does it cost to automate document processing for healthcare providers teams?+
Phased pricing — you commit to one phase at a time. Discovery is $6k for 2-week sprint. Build, scoped from Discovery, runs $20k–$28k over 6-10 weeks. Run is opt-in at $2.5k–$4k / mo per optional, hourly bank also available. ~$32k–$58k typical year 1 (60% take the run option for ~6 months)
What is the best AI agent for document processing in healthcare providers?+
The model is rarely the most consequential choice on document processing in healthcare providers. What matters more: the retrieval shape against your approved sources, the confidence-threshold calibration against the labelled test set, the reviewer queue UX, and the audit log architecture. We benchmark frontier models (Claude, GPT-4-class, Gemini) against your data and select for the accuracy/cost/latency profile that fits your operational reality — not a generic leaderboard.
How long does it take to deploy AI document processing for healthcare providers?+
Production traffic on document processing for healthcare providers typically starts at week 6-8 of Build, after the labelled test set, the eval harness, the reviewer queue, and the audit log are all in place. The first quarter of Run is paired operation — your team takes the dashboard, we stay on the architecture decisions. By the end of the first Run quarter, your team is operating the workflow with the cadence we ship as part of Build.
What do we own, and what do you own?+
The ownership boundary is documented in the Build statement of work. Our side: workflow architecture, prompt library, retrieval shape, evaluation harness, reviewer-queue design, audit log architecture, weekly operating cadence. Your side: data access, source curation by your subject-matter experts, policy interpretation, exception approval, final commercial decisions. Every artefact is yours at the end of Run.
What does Build look like week by week?+
Week 1-2: discovery output, labelled test set, integration plan. Week 3-4: retrieval index live, intake classifier scoring against the test set. Week 5-6: action layer with reviewer approval, thin-slice production traffic. Week 7-10: production envelope widens, calibration tunes against empirical evidence. By end of Build, document processing is operating at its target envelope with the calibration discipline in place.
Do you train models on our data?+
No. We do not train any model on client data. Anthropic Zero-Data-Retention is enabled by default; OpenAI default-no-training is honoured. Prompts, retrieval indexes, audit logs, and integration data live in your cloud account under your IAM. At engagement end, every artefact transfers to your repository.
What if we want to exit the engagement?+
Discovery and Build are fixed-scope, so there is no mid-engagement exit cost. Run is month-to-month with 30-day notice. Every artefact (prompts, eval harness, integration code, dashboards, runbooks) is in your repository throughout the engagement, not behind our SaaS. There is no lock-in.
What does success look like 90 days after Build closes?+
documents per hour, extraction accuracy, exception rate, and processing cost measurably improved against the Discovery baseline. Your team is operating the workflow with the cadence we shipped during Build. The audit log is queryable. The reviewer queue is calibrated. The next workflow scope is informed by real production evidence rather than initial assumptions.
What support is included after the engagement ends?+
Optional Run retainer covers weekly cadence, prompt refresh, retrieval index updates, and reviewer-queue calibration. Architecture-level questions and breaking-change support are billed hourly outside of Run. Most engagements transition Run in-house at month 6-12; we stay available for architecture decisions for 12 months at no extra charge.
How does this integrate with EHR and our existing stack?+
Discovery scopes the integration footprint explicitly. We integrate at the API layer; no replatforming required. The Build statement of work names exactly which systems are connected, which data flows are bidirectional, and what authentication patterns we use (SSO, service accounts, OAuth scopes). The integration code lives in your repository.
What does your team look like during an engagement?+
Discovery: 1 senior delivery lead + 1 PM, ~30 hours/week. Build: 1 senior delivery lead + 2-3 senior AI engineers, ~50-80 hours/week across the team. Run: 1 delivery owner + 1 engineer on weekly cadence. We do not use offshore staff augmentation. Every engineer touching your engagement is senior-level.
Sources we reference
The following sources inform the architecture, governance, and benchmarks we apply on healthcare providers engagements. Cited here so you can verify and dig deeper.
- WHO Artificial Intelligence for Health
- Generative AI in the Enterprise — Deloitte AI Institute
- Worldwide AI and Generative AI Spending Guide — IDC
- Lighthouse Network — Operations AI Adoption — World Economic Forum + McKinsey
- Operations Excellence Through AI — BCG
- Google Search Central: helpful, reliable, people-first content
- Google Search Central: URL structure best practices
Concepts on this page:
AI workflow·Thin slice·Reviewer queue·Evaluation harness·Tool use·Audit logFull glossary →High-intent reads
Start the engagement
Start a Healthcare Providers engagement
Tell us about your workflow, the systems involved, and the KPI you want to move. We'll send a scoped statement of work within 5 business days.